

Cracks in COVID-19 treatment reveal need to bolster primary care
- Written by Tuba Agartan, Associate Professor of Health Policy and Management, Providence College
Every day the COVID-19 crisis reveals just how unprepared[1] the U.S. health care system was.
But it’s not only the shortage of masks, tests and ventilators, nor our chaotic and contradictory public health response, evident across every level of government. COVID-19 has also brought into sharp relief how fragmented and disorganized the American health care system really is.
The U.S. system is often referred to as the dispersed model of care[2] – less structured, with minimal central planning. This model encourages competition over collaboration. Indeed, many patients today can go directly to a specialist without consulting their primary care provider.
COVID-19 has shed light on these organizational problems – and the inability[3] of our health care system to respond to growing demand. As an associate professor[4] of health policy and management working on comparative health systems reforms, I’d like to highlight what primary care can offer in the U.S., especially in the context of a crisis like this one.
 Primary care physicians can provide tremendous front-line support during the pandemic.
Getty Images / Westend61[5]
Primary care physicians can provide tremendous front-line support during the pandemic.
Getty Images / Westend61[5]
The hidden costs of specialty care
While being able to go directly to a specialist may sound like a good deal for the patient, this model has downsides, including higher costs.
That’s in part due to the fact that specialists stay in business by performing diagnostic examinations such as MRI examinations,[6] and surgical procedures, such as coronary artery bypass grafts. And, these specialists compete with each other and try to maximize revenue[7]. The health care industry as a whole spent US$30 billion on advertising[8]. This competitive model encourages provision of high cost services at a higher volume.
These services are not only expensive but are also associated with higher rates of complications and avoidable hospital admissions and readmissions as well as higher rates of hospital-acquired infections. All of these factors point to waste and major inefficiencies[9] in the health care provision and a lack of communication between providers.
How primary care doctors would help
In the current crisis, governors, health officials and the public have placed much attention on 911 and hospital bed capacity[10]. Cities and state governments are coming up with their own response plans without much support from public health agencies and federal government. One example: A fire department battalion chief[11] in Paterson, New Jersey, responded to 911 calls in person to assess possible COVID-19 cases; he determined whether a specialized ambulance should follow up.
Primary care providers could support this triaging work on the front lines and possibly save lives. They also could identify and contact high-risk patients and educate them about the symptoms of COVID-19 before they get sick. They could facilitate at-home testing – of course, depending on the availability of tests. If patients have COVID-19, primary care doctors can manage their care at home through telemedicine or by phone, and refer to hospitals when they get worse.
As the crisis deepens and then abates, primary care doctors will need to educate their patients and encourage behaviors that prevent the spread of disease. And, they can also play a key role for recovering patients in care teams deciding the discharge procedures and help integrate with social care services. These would be essential services for recovering nursing home residents or homeless individuals.
When the system blocks care
But because of our dispersed model, many people[12] don’t even have a primary care doctor. And for those of us who do have them, there is no guarantee that we will be able to receive much needed services.
Some practices are struggling to remain open, due to staff shortages and financial difficulties, while others change their delivery practices such as switching to telemedicine or canceling well and chronic care visits to accommodate need.
A recent survey by Primary Care Collaborative, conducted April 3-6, 2020 with more than 1,000 primary care physicians, nurse practitioners and physician assistants, shows primary care services are “dangerously under-resourced”: [13] 58% of participants report the use of used and homemade personal protective equipment at their practice, while 29% of clinicians report no capacity for COVID-19 testing and 39% have only limited capacity. Nearly half of practices have clinical care team members out sick or quarantined, while 40% report their clinical staff being redeployed within the health system.
The use of telemedicine is growing, but 72% of clinicians reported that “patients most vulnerable do not have capabilities for virtual visits” due to not having a computer or internet access. In addition, 43% of participating clinicians revealed tremendous financial strains threatening practice closure. Especially small, independent practices are struggling with a severe drop in visits, and close to 60% are not sure the majority of care they are provided is reimbursable.
Similarly, community health centers that provide care to medically underserved urban and rural communities are struggling to survive[14].
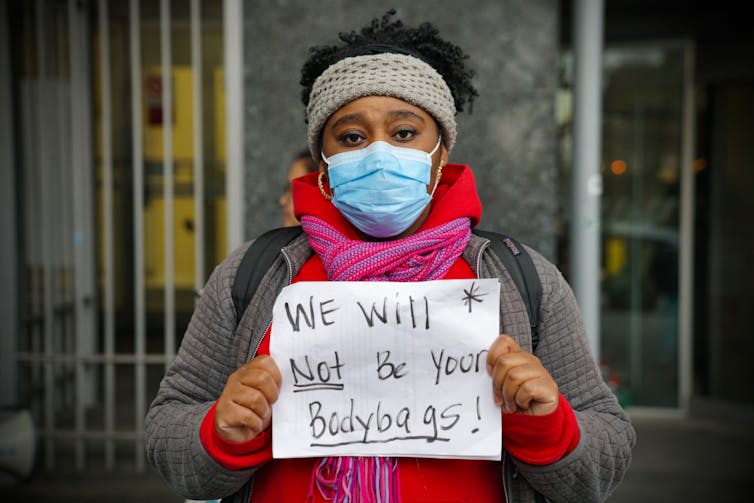 In Harlem, New York, nurses and health care workers protest for more personal protective equipment and safer working conditions. The shortages, says the author, are indicative of an inefficient health care system.
Getty Images / Giles Clarke[15]
In Harlem, New York, nurses and health care workers protest for more personal protective equipment and safer working conditions. The shortages, says the author, are indicative of an inefficient health care system.
Getty Images / Giles Clarke[15]
Reconsider universal health coverage
I do not think that these are just small hiccups. Rather, I think these are the reasons we urgently need a renewed debate on universal health coverage[16], with primary care as its cornerstone.
Various analogies have been used to describe primary care providers, ranging from gatekeepers to quarterbacks. I would suggest another familiar analogy - that of a large, shiny building representing the American health care system. Primary care is often considered as one of the pillars holding the building or the foundation that addresses majority of the health care needs and refers patients to higher levels for complex cases. I would like to add that primary care is also the control center in charge of ensuring an integrated, people-centered system of care.
Primary care system in the U.S. needs to be supported with an organized response that protects the workforce, ensures financial sustainability and facilitates access to accurate information.
To focus on their care management and integration responsibilities, primary care providers need assistance to field questions about COVID-19 symptoms and triaging patients. There are some initiatives we can learn from such as the British health care system’s NHS911[17] hotline or COVID-19 Connected Care Center[18] created in partnership with the Oregon Health & Science University in the U.S.
Our COVID-19 response does not have to be another instance of the “rediscovery[19] of the deficiencies and promises” of our medical and public health systems, but instead, a system-building effort that will better serve us during times of crisis.
[You need to understand the coronavirus pandemic, and we can help. Read The Conversation’s newsletter[20].]
References
- ^ unprepared (www.sciencemag.org)
- ^ dispersed model of care (jamanetwork.com)
- ^ inability (www.aamc.org)
- ^ associate professor (scholar.google.com)
- ^ Getty Images / Westend61 (www.gettyimages.com)
- ^ MRI examinations, (www.healthsystemtracker.org)
- ^ revenue (www.modernhealthcare.com)
- ^ spent US$30 billion on advertising (www.nbcnews.com)
- ^ waste and major inefficiencies (doi.org)
- ^ hospital bed capacity (nashp.org)
- ^ fire department battalion chief (www.nytimes.com)
- ^ many people (www.kff.org)
- ^ primary care services are “dangerously under-resourced”: (www.pcpcc.org)
- ^ survive (www.healthaffairs.org)
- ^ Getty Images / Giles Clarke (www.gettyimages.com)
- ^ universal health coverage (www.who.int)
- ^ NHS911 (111.nhs.uk)
- ^ COVID-19 Connected Care Center (jamanetwork.com)
- ^ rediscovery (www.healthaffairs.org)
- ^ Read The Conversation’s newsletter (theconversation.com)
Authors: Tuba Agartan, Associate Professor of Health Policy and Management, Providence College
Read more https://theconversation.com/cracks-in-covid-19-treatment-reveal-need-to-bolster-primary-care-135413