

Even if you're asymptomatic, COVID-19 can harm your heart, study shows – here's what student athletes need to know
- Written by Partho Sengupta, Abnash C Jain Chair and Professor of Cardiology, Cardiology Division Chief and Director of Cardiac Imaging, West Virginia University
COVID-19 can do some pretty scary things to the human heart. It can trigger blood clots[1] in severe cases and cause inflammation and scarring[2].
New research now shows that even young people with COVID-19 who are asymptomatic are at risk for developing potentially dangerous inflammation around the heart.
I am an imaging cardiologist[3] who is developing diagnostic techniques to assess changes in heart muscle function in patients with COVID-19. In a study released Nov. 4[4], my colleagues and I found evidence of heart abnormalities in over one-third of student athletes who tested positive for COVID-19 and underwent cardiac screening at West Virginia University this fall.
While we didn’t detect ongoing damage to the heart muscle itself, we frequently found evidence of inflammation and excess fluid in the pericardium, the sac around the heart. Almost all of the 54 students tested had either mild COVID-19 or were asymptomatic.
Based on our results and other studies, a group of experts convened by the Journal of the American College of Cardiology: Cardiovascular Imaging has also published a list of recommendations[5] for heart testing and recovery times before student athletes return to play.
An important takeaway: Student athletes who test positive for COVID-19 should consult their primary care physicians to determine if heart screening tests are needed – even if they never showed symptoms.
COVID-19 is bad news for hearts
There is still a lot we don’t know about COVID-19 and its lingering effects on the human body.
SARS-CoV-2, the coronavirus that causes COVID-19, can cause a mind-boggling array of damage[6], including triggering inflammatory responses in the heart muscle and surrounding tissue as the body tries to fight it off. As many as 1 in 8[7] hospitalized COVID-19 patients have some form of heart damage.
What we worry most about with competitive athletes is whether the virus can get into the heart muscle and trigger myocarditis[8], rare inflammation of the heart muscle that can be caused by viral infections. Myocarditis can disrupt your heart’s ability to pump blood[9] and cause arrhythmias. It can also cause sudden heart failure[10] in athletes who seemed healthy. If you have myocarditis, you should not be on the field or in training until well after you recover.
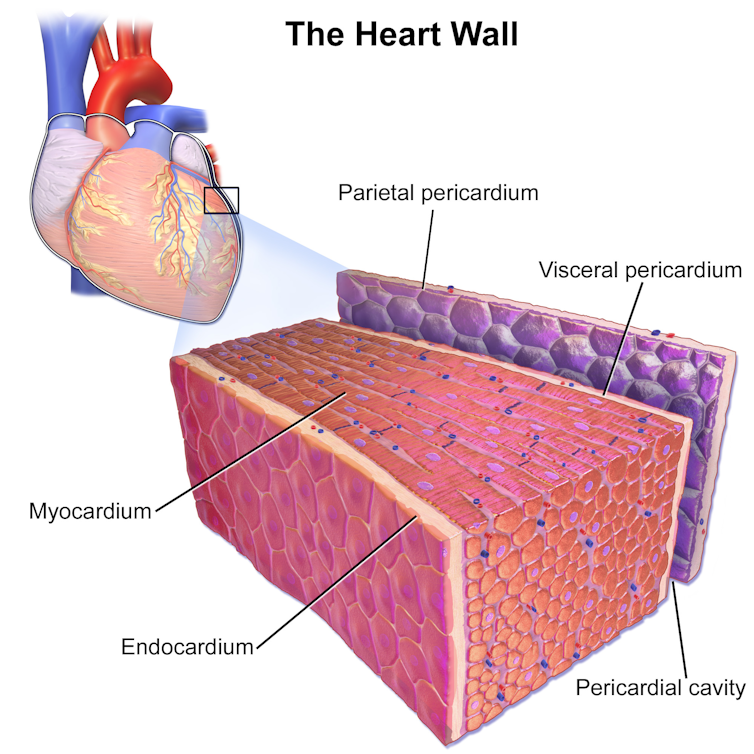 Bruce Blaus/Wikimedia, CC BY[11][12]
A small number of college athletes with COVID-19 are known to have been diagnosed with myocarditis[13]. In one study, Ohio State University doctors tested 26 college athletes in September and found signs of heart inflammation consistent with myocarditis[14] in four.
Myocarditis isn’t the only heart problem to worry about, however. Sports doctors for years have warned that athletes who develop pericarditis should not return to play[15] until it resolves.
Here’s what we found in student athletes
At West Virginia University, my colleagues and I examined 54 student athletes who had tested positive for COVID-19 three to five weeks earlier.
We didn’t find convincing signs of ongoing myocarditis, but we did see a lot of evidence of pericarditis. Among the student athletes screened, 40% had pericardial enhancement, suggesting resolving inflammation in the sac that protects the heart, and 58% had pericardial effusion, meaning excess fluid had built up.
Bruce Blaus/Wikimedia, CC BY[11][12]
A small number of college athletes with COVID-19 are known to have been diagnosed with myocarditis[13]. In one study, Ohio State University doctors tested 26 college athletes in September and found signs of heart inflammation consistent with myocarditis[14] in four.
Myocarditis isn’t the only heart problem to worry about, however. Sports doctors for years have warned that athletes who develop pericarditis should not return to play[15] until it resolves.
Here’s what we found in student athletes
At West Virginia University, my colleagues and I examined 54 student athletes who had tested positive for COVID-19 three to five weeks earlier.
We didn’t find convincing signs of ongoing myocarditis, but we did see a lot of evidence of pericarditis. Among the student athletes screened, 40% had pericardial enhancement, suggesting resolving inflammation in the sac that protects the heart, and 58% had pericardial effusion, meaning excess fluid had built up.
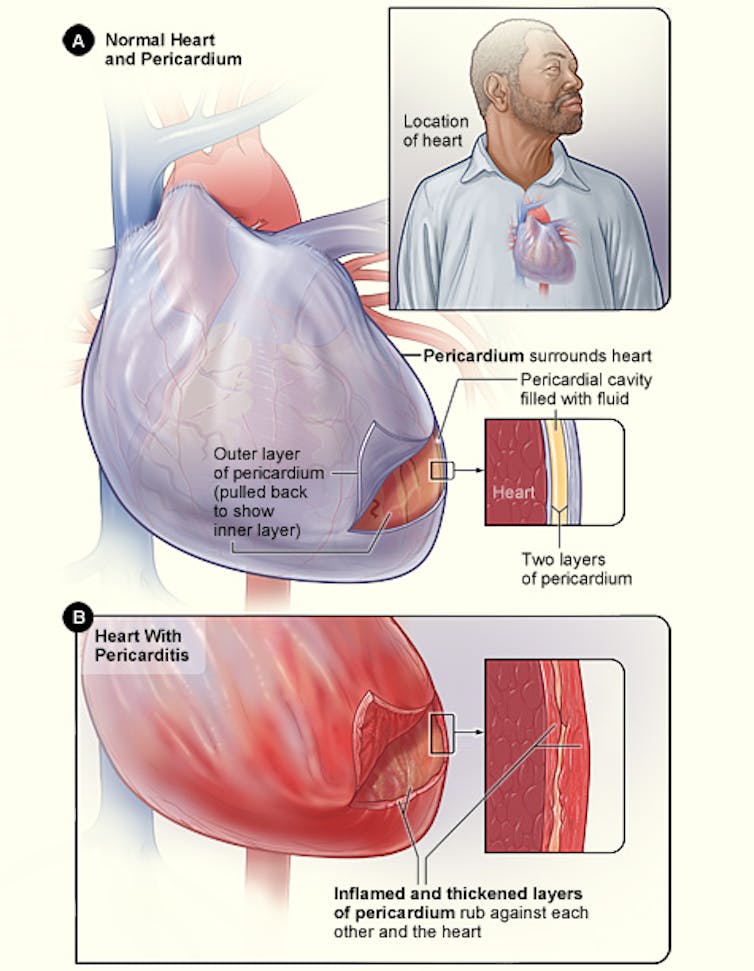 National Heart, Lung and Blood Institute[16]
Usually, this kind of inflammation heals within a few weeks with no residual effects. However, in some cases, there can be long-term effects, like pericardial inflammation recurring. It can lead to scarring of the pericardial sac, which in rare cases can be severe, and the pericardium can constrict around the heart. This can lead to symptoms similar to heart failure and cause congestion in the lungs and liver.
It’s difficult to predict if a patient will develop any of these rare long-term complications, and it’s too soon to tell if it’s happening.
Advice for college athletics programs
Currently, athletic programs around the country have a patchwork of rules for quarantining and screening[17] COVID-19-positive athletes for heart damage as they try to balance players’ health and the desire to return to play.
To help them develop standards, I and other cardiologists from the U.S., Canada, U.K. and Australia reviewed the current evidence and wrote an expert consensus statement[18]. A similar statement[19] focused on myocarditis was published by some of the same doctors in JAMA Cardiology.
We suggest the following:
Any student athlete testing positive for COVID-19 should follow quarantine rules and avoid exposing their teammates, coaches or anyone else to the virus.
Before returning to play, athletes who test positive for COVID-19 should consult with their physicians to determine if heart screening tests are needed. Although routine testing is not recommended for all asymptomatic individuals, a physician should determine on an individual basis when the risks are high enough.
If an athlete has active myocarditis, we recommend no competition or strenuous training for three to six months, with follow-up exams with a cardiologist. Exercise can worsen the disease’s progression and create arrhythmias, or irregular heartbeat. After that period, the athlete can gradually resume exercise and play if he or she has no lingering inflammation or arrhythmia.
If an athlete has active features of pericarditis, we also recommend restricting exercise, since it can exacerbate inflammation or cause inflammation to return. Athletes should avoid competitive sports during the acute phase. Once tests show no inflammation or excess fluid, the athlete should be able to return to play.
[Deep knowledge, daily. Sign up for The Conversation’s newsletter[20].]
COVID-19 is no joke. The best way for athletes to stay healthy so they can keep playing sports is to avoid getting the coronavirus in the first place. Teams should test student athletes for the virus and make sure those who test positive see a doctor to determine if screening tests for heart damage are needed.
National Heart, Lung and Blood Institute[16]
Usually, this kind of inflammation heals within a few weeks with no residual effects. However, in some cases, there can be long-term effects, like pericardial inflammation recurring. It can lead to scarring of the pericardial sac, which in rare cases can be severe, and the pericardium can constrict around the heart. This can lead to symptoms similar to heart failure and cause congestion in the lungs and liver.
It’s difficult to predict if a patient will develop any of these rare long-term complications, and it’s too soon to tell if it’s happening.
Advice for college athletics programs
Currently, athletic programs around the country have a patchwork of rules for quarantining and screening[17] COVID-19-positive athletes for heart damage as they try to balance players’ health and the desire to return to play.
To help them develop standards, I and other cardiologists from the U.S., Canada, U.K. and Australia reviewed the current evidence and wrote an expert consensus statement[18]. A similar statement[19] focused on myocarditis was published by some of the same doctors in JAMA Cardiology.
We suggest the following:
Any student athlete testing positive for COVID-19 should follow quarantine rules and avoid exposing their teammates, coaches or anyone else to the virus.
Before returning to play, athletes who test positive for COVID-19 should consult with their physicians to determine if heart screening tests are needed. Although routine testing is not recommended for all asymptomatic individuals, a physician should determine on an individual basis when the risks are high enough.
If an athlete has active myocarditis, we recommend no competition or strenuous training for three to six months, with follow-up exams with a cardiologist. Exercise can worsen the disease’s progression and create arrhythmias, or irregular heartbeat. After that period, the athlete can gradually resume exercise and play if he or she has no lingering inflammation or arrhythmia.
If an athlete has active features of pericarditis, we also recommend restricting exercise, since it can exacerbate inflammation or cause inflammation to return. Athletes should avoid competitive sports during the acute phase. Once tests show no inflammation or excess fluid, the athlete should be able to return to play.
[Deep knowledge, daily. Sign up for The Conversation’s newsletter[20].]
COVID-19 is no joke. The best way for athletes to stay healthy so they can keep playing sports is to avoid getting the coronavirus in the first place. Teams should test student athletes for the virus and make sure those who test positive see a doctor to determine if screening tests for heart damage are needed.
References
- ^ blood clots (news.weill.cornell.edu)
- ^ cause inflammation and scarring (doi.org)
- ^ imaging cardiologist (scholar.google.com)
- ^ study released Nov. 4 (www.jacc.org)
- ^ published a list of recommendations (doi.org)
- ^ mind-boggling array of damage (theconversation.com)
- ^ 1 in 8 (doi.org)
- ^ myocarditis (www.ncbi.nlm.nih.gov)
- ^ disrupt your heart’s ability to pump blood (www.mayoclinic.org)
- ^ sudden heart failure (doi.org)
- ^ Bruce Blaus/Wikimedia (commons.wikimedia.org)
- ^ CC BY (creativecommons.org)
- ^ diagnosed with myocarditis (www.espn.com)
- ^ consistent with myocarditis (doi.org)
- ^ should not return to play (doi.org)
- ^ National Heart, Lung and Blood Institute (en.wikipedia.org)
- ^ quarantining and screening (www.si.com)
- ^ expert consensus statement (doi.org)
- ^ similar statement (doi.org)
- ^ Sign up for The Conversation’s newsletter (theconversation.com)
Authors: Partho Sengupta, Abnash C Jain Chair and Professor of Cardiology, Cardiology Division Chief and Director of Cardiac Imaging, West Virginia University