

For-profit nursing homes are cutting corners on safety and draining resources with financial shenanigans − especially at midsize chains that dodge public scrutiny
- Written by Sean Campbell, Investigative journalist, The Conversation

The care at Landmark of Louisville Rehabilitation and Nursing was abysmal when state inspectors filed their survey report of the Kentucky facility on July 3, 2021.
Residents wandered the halls[1] in a facility that can house up to 250 people, yelling at each other and stealing blankets. One resident beat a roommate with a stick[2], causing bruising and skin tears. Another was found in bed with a broken finger and a bloody forehead gash[3]. That person was allowed to roam and enter the beds of other residents. In another case, there was sexual touching[4] in the dayroom between residents, according to the report.
Meals were served from filthy meal carts on plastic foam trays, and residents struggled to cut their food with dull plastic cutlery. Broken tiles lined showers, and a mysterious black gunk marred the floors. The director of housekeeping reported that the dining room was unsanitary. Overall, there was a critical lack of training, staff and supervision[5].
The inspectors tagged Landmark as deficient in 29 areas[6], including six that put residents in immediate jeopardy of serious harm and three where actual harm was found. The issues were so severe that the government slapped Landmark with a fine of over $319,000[7] − more than 29 times the average[8] for a nursing home in 2021 − and suspended payments to the home from federal Medicaid and Medicare funds.
Persistent problems
But problems persisted. Five months later, inspectors levied six additional deficiencies of immediate jeopardy − the highest level − including more sexual abuse[10] among residents and a certified nursing assistant pushing someone down, bruising the person’s back and hip.
Landmark is just one of the 58 facilities run by parent company Infinity Healthcare Management across five states. The government issued penalties to the company almost 4½ times the national average, according to bimonthly data that the Centers for Medicare & Medicaid Services first started to make available in late 2022. All told, Infinity paid nearly $10 million in fines[11] since 2021, the highest among nursing home chains with fewer than 100 facilities.
Infinity Healthcare Management and its executives did not respond to multiple requests for comment.
Such sanctions are nothing new[12] for Infinity or other for-profit nursing home chains that have dominated an industry long known for cutting corners in pursuit of profits for private owners. But this race to the bottom to extract profits is accelerating despite demands by government officials[13], health care experts and advocacy groups to protect the nation’s most vulnerable citizens.
To uncover the reasons why, The Conversation’s investigative unit Inquiry delved into the nursing home industry, where for-profit facilities make up more than 72% of the nation’s nearly 14,900 facilities. The probe, which paired an academic expert with an investigative reporter, used the most recent government data on ownership, facility information and penalties, combined with CMS data on affiliated entities for nursing homes.
The investigation revealed an industry that places a premium on cost cutting and big profits, with low staffing and poor quality, often to the detriment of patient well-being. Operating under weak and poorly enforced regulations[14] with financially insignificant penalties, the for-profit sector fosters an environment where corners are frequently cut, compromising the quality of care and endangering patient health. Meanwhile, owners make the facilities look less profitable by siphoning money from the homes through byzantine networks of interconnected corporations. Federal regulators have neglected the problem as each year likely billions of dollars are funneled[15] out of nursing homes through related parties and into owners’ pockets.
More trouble at midsize
Analyzing newly released government data, our investigation found that these problems are most pronounced in nursing homes like Infinity − midsize chains that operate between 11 and 100 facilities[16]. This subsection of the industry has higher average fines per home, lower overall quality ratings, and are more likely to be tagged with resident abuse compared with both the larger and smaller networks. Indeed, while such chains account for about 39% of all facilities, they operate 11 of the 15 most-fined facilities.
With few impediments, private investors who own the midsize chains have quietly swooped in to purchase underperforming homes, expanding their holdings even further as larger chains divest and close facilities. As a result of the industry’s churn of facility ownership[17], over one fifth of the country’s nursing facilities changed ownership between 2016 and 2021, four times more changes than hospitals.
A 2023 report by Good Jobs First, a nonprofit watchdog, noted that a dozen of these chains in the midsize range have doubled or tripled in size[18] while racking up fines averaging over $100,000 per facility since 2018. But unlike the large, multistate chains with easily recognizable names, the midsize networks slip through without the same level of public scrutiny, The Conversation’s investigations unit found.
“They are really bad, but the names − we don’t know these names,” said Toby Edelman, senior policy attorney with the Center for Medicare Advocacy, a nonprofit law organization.
“When we used to have those multistate chains, the facilities all had the same name, so you know what the quality is you’re getting,” she said. “It’s not that good − but at least you know what you’re getting.”
In response to The Conversation’s findings on nursing homes and request for an interview, a CMS spokesperson emailed a statement[19] that said the CMS is “unwavering in its commitment to improve safety and quality of care for the more than 1.2 million residents receiving care in Medicare- and Medicaid-certified nursing homes.”
The statement pointed to data released by the oversight body on mergers, acquisitions, consolidations and changes of ownership[20] in April 2023 along with additional ownership data[21] released the following September. CMS also proposed a rule change that aims to increase transparency in nursing home ownership by collecting more information on facility owners and their affiliations[22].
“Our focus is on advancing implementable solutions that promote safe, high-quality care for residents and consider the challenging circumstances some long-term care facilities face,” the statement reads. “We believe the proposed requirements are achievable and necessary.”
CMS is slated to implement the disclosure rules in the fall and release the new data to the public later this year.
“We support transparency and accountability,” the American Health Care Association/National Center for Assisted Living, a trade organization representing the nursing home industry, wrote in response[23] to The Conversation‘s request for comment. “But neither ownership nor line items on a budget sheet prove whether a nursing home is committed to its residents. Over the decades, we’ve found that strong organizations tend to have supportive and trusted leadership as well as a staff culture that empowers frontline caregivers to think critically and solve problems. These characteristics are not unique to a specific type or size of provider.”
It often takes years to improve a poor nursing home − or run one into the ground[24]. The analysis of midsize chains shows that most owners have been associated with their current facilities for less than eight years, making it difficult to separate operators who have taken long-term investments in resident care from those who are looking to quickly extract money and resources before closing them down or moving on[25]. These chains control roughly 41% of nursing home beds in the U.S., according to CMS’s provider data, making the lack of transparency especially ripe for abuse.
A churn of nursing home purchases even during the COVID-19 pandemic shows that investors view the sector as highly profitable[26], especially when staffing costs are kept low and fines for poor care can easily be covered by the money extracted from residents, their families and taxpayers.
“This is the model of their care: They come in, they understaff and they make their money,” said Sam Brooks, director of public policy at the Consumer Voice, a national resident advocacy organization. “Then they multiply it over a series of different facilities.”
 These pictures showing residents asleep in their food appeared in the 2022 New York attorney general’s lawsuit against The Villages of Orleans Health and Rehabilitation Center in Albion, N.Y.
New York State attorney general's office[27]
These pictures showing residents asleep in their food appeared in the 2022 New York attorney general’s lawsuit against The Villages of Orleans Health and Rehabilitation Center in Albion, N.Y.
New York State attorney general's office[27]
Investor race
The explosion of a billion-dollar private marketplace found its beginnings in government spending.
The adoption of Medicare and Medicaid in 1965 set loose a race among investors to load up on nursing homes, with a surge in for-profit homes gaining momentum because of a reliable stream of government payouts. By 1972, a mere seven years after the inception of the programs, a whopping 106 companies [28]had rushed to Wall Street to sell shares in nursing home companies. And little wonder: They pulled in profits through their ownership of 18% of the industry’s beds, securing about a third of the hefty $3.2 billion of government cash.
The 1990s saw substantial expansion in for-profit nursing home chains, marked by a wave of acquisitions and mergers[29]. At the same time, increasing difficulties emerged in the model for publicly traded chains. Shareholders increasingly demanded[30] rapid growth, and researchers have found[31] that the publicly traded chains tried to appease that hunger by reducing nursing staff and cutting corners on other measures meant to improve quality and safety.
“I began to suspect a possibly inherent contradiction between publicly traded and other large investor-operated nursing home companies and the prerequisites for quality care,” Paul R. Willging, former chief lobbyist for the industry, wrote in a 2007 letter to the editor of The New York Times. “For many investors … earnings growth, quarter after quarter, is often paramount. Long-term investments in quality can work at cross purposes with a mandate for an unending progression of favorable earnings reports.”
One example of that clash can be found at the Ensign Group, founded in 1999 as a private chain of five facilities[32]. Using a strategy of acquiring struggling nursing homes, the company went public in 2007 with more than 60 facilities[33]. What followed was a year-after-year acquisition binge and a track record of growing profits almost every year[34]. Yet the company kept staffing levels below[35] the national average and levels recommended by experts[36]. Its facilities had[37] higher than average inspection deficiencies and higher COVID infection rates. Since 2021, it has racked up more than $6.5 million in penalties[38].
Ensign did not respond to requests for comment.
Even with that kind of expense cutting, not all publicly traded nursing homes survived as the costs of providing poor care added up. Residents sued over mistreatment. Legal fees and settlements ate into profits, shareholders grumbled, and executives searched for a way out of this Catch-22.
Recognizing the long-term potential for profit growth, private investors snapped up publicly traded for-profit chains, reducing the previous levels of public transparency and oversight. Between 2000 and 2017, 1,674 nursing homes were acquired by private-equity firms[39] in 128 unique deals out of 18,485 facilities. But the same poor-quality problems persisted. Research shows that after snagging a big chain, private investors tended to follow the same playbook: They rebrand the company, increase corporate control and dump[40] unprofitable homes to other investment groups willing to take shortcuts for profit.
Multiple[41] academic[42] studies[43] show the results, highlighting the lower staffing and quality in for-profit homes compared with nonprofits and government-run facilities. Elderly residents staying long term in nursing homes owned by private investment groups experienced a significant uptick[44] in trips to the emergency department and hospitalizations between 2013 and 2017, translating into higher costs for Medicare.
Overall, private-equity investors wreak havoc[45] on nursing homes, slashing registered nurse hours per resident day by 12%, outpacing other for-profit facilities. The aftermath is grim, with a daunting 14% surge in the deficiency score index, a standardized metric for determining issues with facilities, according to a U.S. Department of Health and Human Services report.
The human toll comes in death and suffering. A study updated in 2023 by the National Bureau of Economic Research calculated that 22,500 additional deaths[46] over a 12-year span were attributable to private-equity ownership, equating to about 172,400 lost life years. The calculations also showed that private-equity ownership was responsible for a 6.2% reduction in mobility, an 8.5% increase in ulcer development and a 10.5% uptick in pain intensity.
Hiding in complexity
Exposing the identities of who should be held responsible for such anguish poses a formidable task. Private investors in nursing home chains often employ a convoluted system[47] of limited liability corporations, related companies and family relationships to obscure who controls[48] the nursing homes.
These adjustments are crafted to minimize liability, capitalize on favorable tax policies, diminish regulatory scrutiny and disguise nursing home profitability. In this investigation, entities at every level of involvement with a nursing home denied ownership, even though the same people controlled each organization.
A rule put in place in 2023[49] by the Centers for Medicare & Medicaid Services requires the identification of all private-equity and real estate investment trust investors in a facility and the release of all related party names. But this hasn’t been enough to surface the players and relationships. More than half of ownership data provided to CMS is incomplete across all facilities, according to a March 2024 analysis[50] of the newly released data.
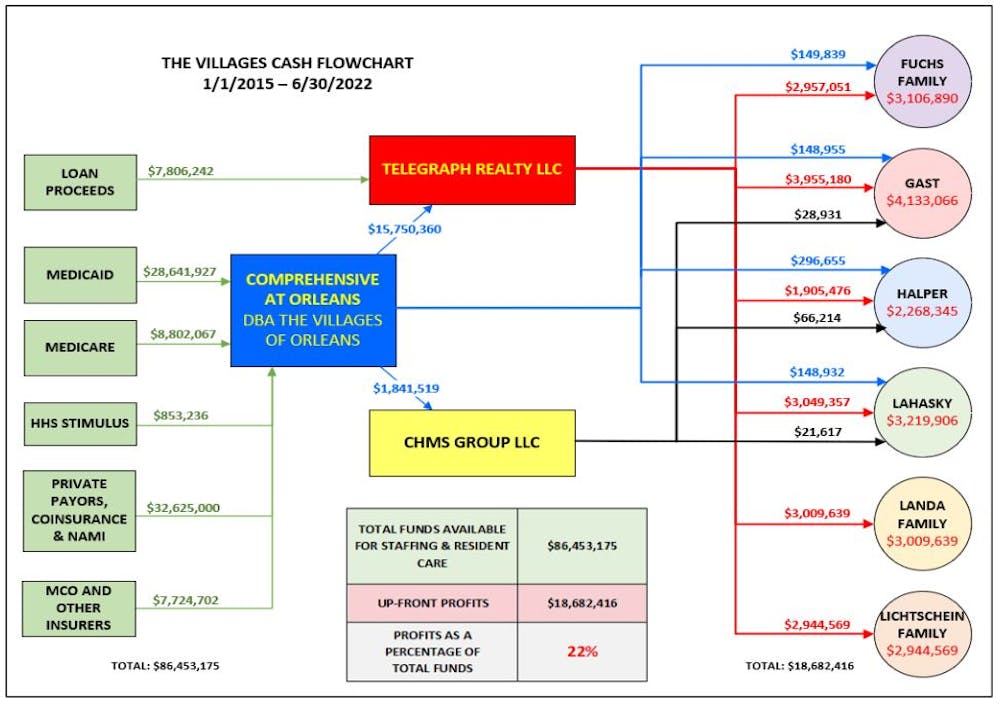 Nursing home investors drained more than $18 million out of a single facility through a complex web of related party transactions.
New York State attorney general's office[51]
Nursing home investors drained more than $18 million out of a single facility through a complex web of related party transactions.
New York State attorney general's office[51]
Even the land under the nursing home is often owned by someone else. In 2021, publicly traded or private real estate investment trusts held a sizable chunk[52] of the approximately $120 billion of nursing home real estate. As with homes owned by private-equity investors, quality measures collapse[53] after REITs get involved, with facilities witnessing a 7% decline in registered nurses’ hours per resident day and an alarming 14% ascent in the deficiency score index. It’s a blatant pattern of disruption, leaving facilities and care standards in a dire state.
Part of that quality collapse comes from the way these investment entities make their money. REITs and their owners can drain cash out[54] of the nursing homes in a number of different ways. The standard tactic for grabbing the money is known as a triple-net lease, where the REIT buys the property then leases it back to the nursing home, often at exorbitant rates[55]. Although the nursing home then lacks possession of the property, it still gets slammed with costs typically shouldered by an owner − real estate taxes, insurance, maintenance and more. Topping it off, the facilities then must typically pay annual rent hikes.
A second tactic that REITs use involves a contracting façade that serves no purpose other than enriching the owners of the trusts. Since triple-net lease agreements prohibit REITs from taking profits from operating the facilities, the investors create a subsidiary to get past that hurdle. The subsidiary then contracts with a nursing home operator − often owned or controlled by another related party − and then demands a fee for providing operational guidance. The use of REITs for near-risk-free profits from nursing homes has proven to be an ever-growing technique, and the midsize chains[56], which our investigation found generally provided the worst care, grew in their reliance on REITs during the pandemic.
“When these REITs start coming in … nursing homes are saddled with these enormous rents, and then they wind up going out of business,” said Richard Mollot, executive director of the Long-Term Care Community Coalition[57], a nonprofit organization that advocates for better care at nursing homes. “It’s no longer a viable facility.”
The churn of nursing home purchases by midsize chains underscores investors’ perception of the sector’s profitability, particularly when staffing expenses are minimized and penalties for subpar care can be offset by money extracted through related transactions and payments from residents, their families and taxpayers. Lawsuits can drag out over years, and in the worst case, if a facility is forced to close, its land and other assets can be sold to minimize the financial loss.
Take Brius Healthcare, a name that resonates with a disturbing cadence in the world of nursing home ownership. A search of the federal database for nursing home ownership and penalties shows that Brius was responsible for 32 facilities[58] as of the start of 2024, but the true number is closer to 80[59], according to BriusWatch.org, which tracks violations. At the helm of this still midsize network stands Shlomo Rechnitz, who became a billionaire in part by siphoning from government payments[60] to his facilities scattered across California, according to a federal and state lawsuit.
In lawsuits[61] and regulators’ criticisms, Rechnitz’s homes have been associated[62] with tales of abuse, as well as several lawsuits alleging terrible care. The track record was so bad that, in the summer of 2014, then-California Attorney General Kamala Harris filed an emergency motion[63] to block Rechnitz from acquiring 19 facilities, writing that he was “a serial violator of rules within the skilled nursing industry” and was “not qualified to assume such an important role.”
Yet, Rechnitz’s empire in California surged forward, scooping up more facilities that drained hundreds of millions of federal and state funds as they racked up pain and profit[64]. The narrative played out at Windsor Redding Care Center in Redding, California. Rechnitz bought it from a competing nursing home chain and attempted to obtain a license to operate the facility. But in 2016, the California Department of Public Health refused the application[65], citing a staggering 265 federal regulatory violations across his other nursing homes over just three years.
According to court filings, Rechnitz formed a joint venture with other investors[66] who in turn held the license. Rechnitz, through the Brius joint venture, became the unlicensed owner and operator of Windsor Redding.
Brius carved away at expenses, slashing staff and other care necessities[67], according to a 2022 California lawsuit. One resident was left to sit in her urine and feces for hours at a time. Overwhelmed staff often did not respond to her call light, so once she instead climbed out of bed unassisted, fell and fractured her hip. Other negligence led to pressure ulcers, and when she was finally transferred to a hospital, she was suffering from sepsis. She was not alone in her suffering. Numerous other residents[68] experienced an unrelenting litany of injuries and illnesses, including pressure ulcers, urinary tract infections from poor hygiene, falls, and skin damage from excess moisture, according to the lawsuit.
In 2023, California moved forward with licensing two dozen[69] of Rechnitz’s facilities with an agreement that included a two-year monitoring period, right before statewide reforms[70] were set to take effect. The reforms don’t prevent existing owners like Rechnitz from continuing to run a nursing home without a license, but they do prevent new operators from doing so.
“We’re seeing more of that, I think, where you have a proliferation of really bad operators that keep being provided homes,” said Brooks, the director of public policy at the Consumer Voice. “There’s just so much money to be made here for unscrupulous people, and it just happens all the time.”
Rechnitz did not respond to multiple requests for comment. Bruis also did not respond.
Perhaps no other chain showcases the havoc that can be caused by one individual’s acquisition of multiple nursing homes than Skyline Health Care[71]. The company’s owner, Joseph Schwartz, parlayed the sale of his insurance business into ownership of 90 facilities between mid-2016 and December 2017, according to a federal indictment[72]. He ran the company out of an office above a New Jersey pizzeria[73] and at its peak managed facilities in 11 states.
Schwartz went all-in on cost cutting, and by early 2018, residents were suffering from the shortage of staff. The company wasn’t paying its bills[74] or its workers[75]. More than a dozen lawsuits piled up. Last year, Schwartz was arrested and faced charges in federal district court in New Jersey for his role in a $38 million payroll tax scheme[76]. In 2024, Schwartz pleaded guilty[77] to his role in the fraud scheme. He is awaiting sentencing, where he faces a year in prison[78] along with paying at least $5 million in restitution.
Skyline collapsed and disrupted thousands of lives[79]. Some states took over facilities; others closed, forcing residents to relocate and throwing families into chaos. The case also highlights the ease with which some bad operators can snap up nursing homes with little difficulty, with federal and state governments allowing ownership changes with little or no review.
Schwartz’s lawyer did not respond to requests for comment.
Not that nursing homes have much to fear in the public perception of their reputation for quality. CMS uses what is known as the Five-Star Quality Rating System[80], designed to help consumers compare nursing homes to find one that provides good care. Theoretically, nursing homes with five-star ratings are supposed to be exceptional, while those with one-star ratings are deemed the worst. But research shows that nursing homes can game the system[81], with the result that a top star rating might reflect little more than a facility’s willingness to cheat.
A star rating is composed of three parts: The score from a government inspection and the facility’s self-reports of staffing and quality. This means that what the nursing homes say about themselves can boost the star rating of facilities even if they have poor inspection results.
Multiple studies[82] have highlighted a concerning trend: Some nursing homes, especially for-profit ones, inflate their self-reported measures[83], resulting in a disconnect from actual inspection findings. Notably, research suggests that for-profit nursing homes, driven by significant financial motives, are more likely to engage in this practice of inflating their self-reported assessments.
At bottom, the elderly and their families seeking quality care unknowingly find themselves in an impossible situation with for-profit nursing homes: Those facilities tend to provide the worst quality, and the only measure available for consumers to determine where they will be treated well can be rigged. The result is the transformation of an industry meant to care for the most vulnerable into a profit-driven circus.
 The for-profit nursing home sector is growing, and it places a premium on cost cutting and big profits, which has led to low staffing and patient neglect and mistreatment.
picture alliance via Getty Images[84]
The for-profit nursing home sector is growing, and it places a premium on cost cutting and big profits, which has led to low staffing and patient neglect and mistreatment.
picture alliance via Getty Images[84]
The pandemic
Nothing more clearly exposed the problems rampant in nursing homes than the pandemic. Throughout that time, nursing homes reported[85] that almost 2 million residents had infections and 170,000 died.
No one should have been surprised by the mass death in nursing homes − the warning signs of what was to come had been visible for years. Between 2013 and 2017, infection control was the most frequently cited deficiency[86] in nursing homes, with 40% of facilities cited each year and 82% cited at least once in the five-year period. Almost half were cited over multiple consecutive years for these deficiencies − if fixed, one of the big causes of the widespread transmission of COVID in these facilities would have been eliminated.
But shortly after coming into office in 2017, the Trump administration weakened what was already a deteriorating system to regulate nursing homes. The administration directed regulators to issue one-time fines[87] against nursing homes for violations of federal rules rather than for the full time they were out of compliance. This shift meant that even nursing homes with severe infractions lasting weeks were exempted from fines surpassing the maximum per-instance penalty of $20,965.
Even that near-worthless level of regulation was not feeble enough for the industry, so lobbyists pressed for less. In response, just a few months before COVID emerged in China, the Trump administration implemented new regulations[88] that effectively abolished a mandate for each to hire a full-time infection control expert, instead recommending outside consultants[89] for the job.
The perfect storm had been reached, with no experts required to be on site, prepared to combat any infection outbreaks. On Jan. 20, 2020 − just 186 days after the change in rules on infection control − the CDC reported that the first[90] laboratory-confirmed case of COVID had been found at a nursing home in Washington state.
The least prepared in this explosion of disease were the for-profit nursing homes, compared with nonprofit and government facilities. Research from the University of California at San Francisco found those facilities were linked to higher numbers[91] of COVID cases. For-profits not only had fewer nurses on staff but also high numbers of infection-control deficiencies and lower compliance with health regulations.
Even as the United States went through the crisis, some owners of midsize chains continued snapping up nursing homes. For example, two Brooklyn businessmen named Simcha Hyman and Naftali Zanziper were going on a nursing home buying spree[92] through their private-equity company, the Portopiccolo Group. Despite poor ratings[93] in their previously owned facilities, nothing blocked the acquisitions.
One such facility was a struggling nursing home in North Carolina now known as The Citadel Salisbury. Following the traditional pattern forged by private investors in the industry, the new owners set up a convoluted network of business[94] entities and then used them to charge the nursing home for services and property. A 2021 federal lawsuit of many plaintiffs claimed that they deliberately kept the facility understaffed[95] and undersupplied to maximize profit.
Within months of the first case of COVID reported in America, The Citadel Salisbury experienced the largest nursing home outbreak in the state. The situation was so dire that on April 20, 2020, the local medical director of the emergency room took to the local newspaper[96] to express his distress, revealing that he had pressed the facility’s leadership and the local health department to address the known shortcomings.
The situation was “a blueprint for exactly what not to do in a crisis,” medical director John Bream wrote. “Patients died at the Citadel without family members being notified. Families were denied the ability to have one last meaningful interaction with their family. Employees were wrongly denied personal protective equipment. There has been no transparency.”
After a series of scathing inspection reports[97], the facility finally closed[98] in the spring of 2022. As for the federal lawsuit, court documents show that a tentative agreement was reached in 2023. But the case dragged out for nearly three years, and one of the plaintiffs, Sybil Rummage, died while seeking accountability[99] through the court.
Still, the pandemic had been a time of great success for Hyman and Zanziper. At the end of 2020, they owned more than 70 facilities. By 2021, their portfolio had exploded to more than 120. Now, according to data from the Centers for Medicare & Medicaid Services, Hyman and Zanziper are associated with at least 131 facilities and have the highest amount of total fines recorded by the agency for affiliated entities, totaling nearly $12 million since 2021. And their average fine per facility, as calculated by CMS, is more than twice the national average[100] at almost $90,000.
In a written statement[101], Portopiccolo Group spokesperson John Collins disputed that the facilities had skimped on care and argued that they were not managed by the firm. “We hire experienced, local health care teams who are in charge of making all on-the-ground decisions and are committed to putting residents first.” He added that the number of facilities given by CMS was inaccurate but declined to say how many are connected to its network of affiliates or owned by Hyman and Zanziper.
With the nearly 170,000 resident deaths from COVID and many related fatalities from isolation and neglect in nursing homes, in February 2022 President Biden announced an initiative[102] aimed at improving the industry. In addition to promising to set a minimum staffing standard, the initiative is focused on improving ownership and financial transparency.
“As Wall Street firms take over more nursing homes, quality in those homes has gone down and costs have gone up. That ends on my watch,” Biden said during his 2022 State of the Union address. “Medicare is going to set higher standards for nursing homes and make sure your loved ones get the care they deserve and expect.”
 President Joe Biden signed an executive order on April 18, 2023, that directed the secretary of health and human services to consider actions that would build on nursing home minimum staffing standards and improve staff retention.
Nathan Posner/Anadolu Agency via Getty Images[103]
President Joe Biden signed an executive order on April 18, 2023, that directed the secretary of health and human services to consider actions that would build on nursing home minimum staffing standards and improve staff retention.
Nathan Posner/Anadolu Agency via Getty Images[103]
Still, the current trajectory of actions[104] appears to fall short of what’s needed. While penalties against facilities have sharply increased under Biden, some of the Trump administration’s weak regulations have not been replaced.
A rule[105] proposed by CMS in September 2023 and released for review[106] in March 2024 would require states to report what percentage of Medicaid funding is used to pay direct care workers and support staff and would require an RN on duty 24/7. It would also require a minimum of three hours[107] of skilled staffing care per patient per day. But the three-hour minimum is substantially lower than the 4.1 hours of skilled staffing for nursing home residents suggested by CMS over two decades ago[108].
The requirements are also lower than the 3.8 average nursing staff hours[109] already employed by U.S. facilities.
The current administration has also let stand the Trump administration reversal[110] of an Obama rule that banned binding arbitration agreements in nursing homes.
It breaks a village
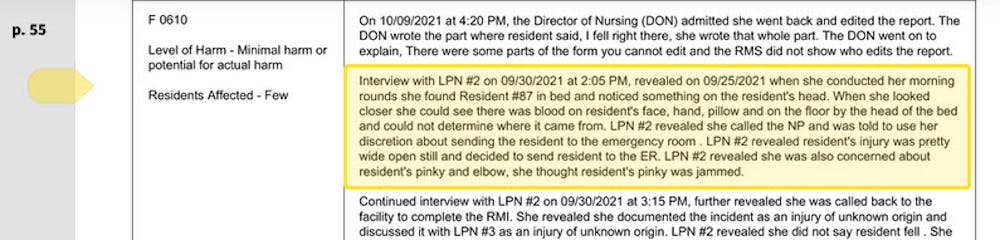
The Villages of Orleans Health and Rehabilitation Center in Albion, New York, was, by any reasonable measure, broken. Court records show that on some days there was no nurse and no medication[111] for the more than 100 elderly residents. Underpaid staff spent their own cash for soap[112] to keep residents clean. At times, the home didn’t feed[113] its frail occupants.
Meanwhile, according to a 2022 lawsuit filed by the New York attorney general, riches were siphoned out of the nursing home[114] and into the pockets of the official owner, Bernard Fuchs, as well as assorted friends, business associates and family. The lawsuit says $18.7 million flowed from the facility to entities owned by a group of men who controlled the Village’s operations.
Although these men own various nursing homes, Medicare records show few connections between them, despite them all being investors in Comprehensive Healthcare Management, which provided administrative services to the Villages. Either they or their families were also owners of Telegraph Realty, which leased what was once the Villages’ own property back[115] to the facility at rates the New York attorney general deemed exorbitant, predatory and a sham.
So it goes in the world of nursing home ownership, where overlapping entities and investors obscure the interrelationships between them to such a degree that Medicare itself is never quite sure who owns what.
Glenn Jones, a lawyer representing Comprehensive Healthcare Management, declined to comment on the pending litigation, but he forwarded a court document his law firm filed[116] that labels the allegations brought by the New York attorney general “unfounded” and reliant on “a mere fraction” of its residents.
 These pictures of the same resident one month apart at the Holliswood Center for Rehabilitation and Healthcare in Queens appeared in a 2023 New York attorney general lawsuit against 13 LLCs and 14 individuals. The group owns multiple nursing homes and allegedly neglected residents, while owners siphoned Medicare and Medicaid money into their own pockets.
New York attorney general's office[117]
These pictures of the same resident one month apart at the Holliswood Center for Rehabilitation and Healthcare in Queens appeared in a 2023 New York attorney general lawsuit against 13 LLCs and 14 individuals. The group owns multiple nursing homes and allegedly neglected residents, while owners siphoned Medicare and Medicaid money into their own pockets.
New York attorney general's office[117]
The shadowy structure of ownership and related party transactions plays an enormous role in how investors enrich themselves, even as the nursing homes they control struggle financially. Compounding the issue, the figures reported by nursing homes regarding payments to related parties frequently diverge[118] from the disclosures made by the related parties themselves.
As an illustration of the problems, consider Pruitt Health[119], a midsize chain with 87 nursing homes[120] spread across Georgia, South Carolina, North Carolina and Florida that had low overall federal quality ratings and about $2 million in penalties. A report by The National Consumer Voice For Quality Long-Term Care, a consumer advocacy group, shows that Pruitt disclosed[121] general related party costs nearing $482 million from 2018 to 2020. Yet in that same time frame, Pruitt reported payments to specific related parties amounting to about $570 million, indicating a $90 million excess. Its federal disclosures offer no explanation for the discrepancy. Meanwhile, the company reported $77 million in overall losses on its homes.
The same pattern holds in the major chains such as the Cleveland, Tennessee-based Life Care Centers of America, which operates roughly 200 nursing homes across 27 states, according to the report. Life Care’s financial disbursements are fed into a diverse spectrum of related entities, including management, staffing, insurance and therapy companies, all firmly under the umbrella of the organization’s ownership. In fiscal year 2018, the financial commitment to these affiliated entities reached $386,449,502; over the three-year period from 2018 to 2020, Life Care’s documented payments to such parties hit an eye-popping $1.25 billion.
Pruitt Health and Life Care Centers did not respond to requests for comment.
Overall, 77% of US nursing homes reported $11 billion[122] in related-party transactions in 2019 − nearly 10% of total net revenues − but the data is unaudited and unverified. The facilities are not required to provide any details[123] of what specific services were provided by the related parties, or what were the specific profits and administrative costs, creating a lack of transparency regarding expenses that are ambiguously categorized under generic labels such as “maintenance.” Significantly, there is no mandate to disclose whether any of these costs exceed fair market value.
What that means is that nursing home owners can profit handsomely through related parties even if their facilities are being hit with repeated fines for providing substandard care.
“What we would consider to be a big penalty really doesn’t matter because there’s so much money coming in,” said Mollot of the Long-Term Care Community Coalition. “If the facility fails, so what? It doesn’t matter. They pulled out the resources.’’
Hiding profit
Ultimately, experts say, this ability to drain cash out of nursing homes makes it almost impossible for anyone to assess the profitability of these facilities based on their public financial filings, known as cost reports.
"The profit margins (for nursing homes) also should be taken with a grain of salt in the cost reports,” said Dr. R. Tamara Konetzka, a University of Chicago professor of public health sciences, at a recent meeting[124] of the Medicare Payment Advisory Commission[125]. “If you sell the real estate to a REIT or to some other entity, and you pay sort of inflated rent back to make your profit margins look lower, and then you recoup that profit because it’s a related party, we’re not going to find that in the cost reports.”
That ability to hide profits is key to nursing homes’ ability to block regulations to improve quality of care and to demand greater government payments. For decades, the industry’s refrain[126] has been that cuts in reimbursements or requirements to increase staffing will drive facilities into bankruptcy; already, they claim, half of all nursing homes are teetering on the edge of collapse, the result, they say, of inadequate Medicaid rates[127]. All in all, the industry reports that less than 3%[128] of their revenue goes to earnings.
But that does not include any of the revenue pulled out of the homes to boost profits of related parties controlled by the same owners pleading poverty. And this tactic is only one of several ways that the nursing home industry disguises its true profits, giving it the power to plead poverty to an unknowing government.
Under the regulations, only certain nursing home expenses are reimbursable[129], such as money spent for care. Many others − unreasonable payments to the headquarters of chains, luxury items, and fees for lobbyists and lawyers − are disallowed after Medicare reviews the cost reports. But by that time, the government has already reimbursed the nursing homes for those expenses − and none of those revenues have to be returned[130].
Data indicates that owners also profit by overcharging nursing homes for services and leases provided by related entities. A March 2024 study from Lehigh University and the University of California, Los Angeles shows that costs were inflated[131] when nursing home owners changed from independent contractors to businesses owned or controlled directly or indirectly by the same people. Overall, spending on real estate increased 20.4%, and spending on management increased 24.6% when the businesses were affiliated, the research showed.
Nursing homes also claim that noncash depreciation cuts into their profits[132]. Those expenses, which show up only in accounting ledgers, assume that assets such as equipment and facilities are gradually decreasing in value and ultimately will need to be replaced.
That might be reasonable if the chains purchased new items once their value depreciated to zero, but that is not always true. A 2004 report[133] by the Medicare Payment Advisory Commission found that the depreciation claimed by health care companies, including nursing homes, may not reflect actual capital expenditures or the actual market value.
If disallowed expenses and noncash depreciation were not included, profit margins for the nursing home industry would jump[134] to 8.8%, far more than the 3% it claims. And given that these numbers all come from nursing home cost reports submitted to the government, they may underestimate the profits even more. Audited cost reports are not required, and the Government Accountability Office has found[135] that CMS does little to ensure the numbers are correct and complete.
This lack of basic oversight essentially gives dishonest nursing home owners the power to grab more money from Medicare and Medicaid while being empowered to claim that their financials prove they need more.
“They face no repercussions,” Brooks of Consumer Voice said, commenting on the current state of nursing home operations and their unscrupulous owners. “That’s why these people are here. It’s a bonanza to them.”
Ultimately, experts say, finding ways to force nursing homes to provide quality care has remained elusive. Michael Gelder, former senior health policy adviser to then-Gov. Pat Quinn of Illinois, learned that brutal lesson in 2010 as head of a task force formed by Quinn to investigate nursing home quality. That group successfully pushed a new law, but Gelder now says his success failed to protect this country’s most vulnerable citizens.
“I was perhaps naively convinced that someone like myself being in the right place at the right time with enough resources could really fix this problem,” he said. “I think we did the absolute best we could, and the best that had ever been done in modern history up to that point. But it wasn’t enough. It’s a battle every generation has to fight.”
Click to learn more about how some existing tools[136] can address problems with for-profit nursing homes.
References
- ^ wandered the halls (www.documentcloud.org)
- ^ with a stick (www.documentcloud.org)
- ^ gash (www.documentcloud.org)
- ^ sexual touching (www.documentcloud.org)
- ^ supervision (projects.propublica.org)
- ^ deficient in 29 areas (medicare.gov)
- ^ a fine of over $319,000 (www.medicare.gov)
- ^ more than 29 times the average (data.cms.gov)
- ^ New York State attorney general's office (www.medicare.gov)
- ^ more sexual abuse (www.documentcloud.org)
- ^ nearly $10 million in fines (data.cms.gov)
- ^ sanctions are nothing new (violationtracker.goodjobsfirst.org)
- ^ government officials (www.gao.gov)
- ^ weak and poorly enforced regulations (deliverypdf.ssrn.com)
- ^ each year likely billions of dollars are funneled (theconsumervoice.org)
- ^ operate between 11 and 100 facilities (data.cms.gov)
- ^ churn of facility ownership (aspe.hhs.gov)
- ^ doubled or tripled in size (goodjobsfirst.org)
- ^ a statement (www.documentcloud.org)
- ^ mergers, acquisitions, consolidations and changes of ownership (www.hhs.gov)
- ^ additional ownership data (www.hhs.gov)
- ^ collecting more information on facility owners and their affiliations (www.federalregister.gov)
- ^ wrote in response (www.documentcloud.org)
- ^ run one into the ground (www.newyorker.com)
- ^ before closing them down or moving on (www.wpr.org)
- ^ highly profitable (doi.org)
- ^ New York State attorney general's office (ag.ny.gov)
- ^ 106 companies (babel.hathitrust.org)
- ^ acquisitions and mergers (aspe.hhs.gov)
- ^ Shareholders increasingly demanded (www.jstor.org)
- ^ researchers have found (www.ncbi.nlm.nih.gov)
- ^ founded in 1999 as a private chain of five facilities (www.sec.gov)
- ^ went public in 2007 with more than 60 facilities (www.sec.gov)
- ^ profits almost every year (journals.sagepub.com)
- ^ kept staffing levels below (journals.sagepub.com)
- ^ levels recommended by experts (www.justice.gov)
- ^ Its facilities had (journals.sagepub.com)
- ^ $6.5 million in penalties (data.cms.gov)
- ^ acquired by private-equity firms (doi.org)
- ^ rebrand the company, increase corporate control and dump (doi.org)
- ^ Multiple (doi.org)
- ^ academic (dx.doi.org)
- ^ studies (doi.org)
- ^ a significant uptick (doi.org)
- ^ wreak havoc (aspe.hhs.gov)
- ^ calculated that 22,500 additional deaths (doi.org)
- ^ convoluted system (doi.org)
- ^ to obscure who controls (theconsumervoice.org)
- ^ rule put in place in 2023 (www.federalregister.gov)
- ^ March 2024 analysis (www.healthaffairs.org)
- ^ New York State attorney general's office (ag.ny.gov)
- ^ held a sizable chunk (doi.org)
- ^ quality measures collapse (aspe.hhs.gov)
- ^ can drain cash out (doi.org)
- ^ at exorbitant rates (ssrn.com)
- ^ the midsize chains (aspe.hhs.gov)
- ^ Long-Term Care Community Coalition (nursinghome411.org)
- ^ responsible for 32 facilities (data.cms.gov)
- ^ closer to 80 (briuswatch.org)
- ^ by siphoning from government payments (www.documentcloud.org)
- ^ In lawsuits (s3.documentcloud.org)
- ^ have been associated (briuswatch.org)
- ^ emergency motion (www.scribd.com)
- ^ racked up pain and profit (www.washingtonpost.com)
- ^ refused the application (canhr.org)
- ^ a joint venture with other investors (www.documentcloud.org)
- ^ slashing staff and other care necessities (www.documentcloud.org)
- ^ Numerous other residents (www.documentcloud.org)
- ^ licensing two dozen (calmatters.org)
- ^ right before statewide reforms (calmatters.org)
- ^ Skyline Health Care (skillednursingnews.com)
- ^ federal indictment (www.documentcloud.org)
- ^ above a New Jersey pizzeria (www.govinfo.gov)
- ^ wasn’t paying its bills (www.medicareadvocacy.org)
- ^ workers (www.mass.gov)
- ^ $38 million payroll tax scheme (www.justice.gov)
- ^ pleaded guilty (www.justice.gov)
- ^ faces a year in prison (www.documentcloud.org)
- ^ disrupted thousands of lives (www.nbcnews.com)
- ^ Five-Star Quality Rating System (www.cms.gov)
- ^ can game the system (doi.org)
- ^ Multiple studies (nihcm.org)
- ^ inflate their self-reported measures (doi.org)
- ^ picture alliance via Getty Images (www.gettyimages.com)
- ^ nursing homes reported (data.cms.gov)
- ^ most frequently cited deficiency (www.gao.gov)
- ^ directed regulators to issue one-time fines (www.nytimes.com)
- ^ implemented new regulations (www.federalregister.gov)
- ^ recommending outside consultants (www.americanprogress.org)
- ^ reported that the first (www.cdc.gov)
- ^ linked to higher numbers (doi.org)
- ^ buying spree (pe-insights.com)
- ^ Despite poor ratings (www.washingtonpost.com)
- ^ convoluted network of business (www.documentcloud.org)
- ^ kept the facility understaffed (www.classaction.org)
- ^ took to the local newspaper (www.salisburypost.com)
- ^ series of scathing inspection reports (www.documentcloud.org)
- ^ facility finally closed (www.cms.gov)
- ^ died while seeking accountability (www.documentcloud.org)
- ^ more than twice the national average (data.cms.gov)
- ^ written statement (www.documentcloud.org)
- ^ announced an initiative (www.whitehouse.gov)
- ^ Nathan Posner/Anadolu Agency via Getty Images (www.gettyimages.com)
- ^ current trajectory of actions (www.whitehouse.gov)
- ^ rule (www.reginfo.gov)
- ^ released for review (www.reginfo.gov)
- ^ require an RN on duty 24/7. It would also require a minimum of three hours (www.cms.gov)
- ^ suggested by CMS over two decades ago (www.justice.gov)
- ^ 3.8 average nursing staff hours (data.cms.gov)
- ^ Trump administration reversal (www.cms.gov)
- ^ on some days there was no nurse and no medication (www.documentcloud.org)
- ^ spent their own cash for soap (www.documentcloud.org)
- ^ didn’t feed (www.documentcloud.org)
- ^ riches were siphoned out of the nursing home (www.documentcloud.org)
- ^ leased what was once the Villages’ own property back (www.documentcloud.org)
- ^ court document his law firm filed (www.documentcloud.org)
- ^ New York attorney general's office (ag.ny.gov)
- ^ frequently diverge (theconsumervoice.org)
- ^ Pruitt Health (pruitthealth.com)
- ^ 87 nursing homes (data.cms.gov)
- ^ shows that Pruitt disclosed (theconsumervoice.org)
- ^ 77% of US nursing homes reported $11 billion (journals.sagepub.com)
- ^ are not required to provide any details (theconsumervoice.org)
- ^ recent meeting (nursinghome411.org)
- ^ Medicare Payment Advisory Commission (www.medpac.gov)
- ^ industry’s refrain (www.ahcancal.org)
- ^ the result, they say, of inadequate Medicaid rates (www.ahcancal.org)
- ^ less than 3% (www.ahcancal.org)
- ^ only certain nursing home expenses are reimbursable (journals.sagepub.com)
- ^ none of those revenues have to be returned (doi.org)
- ^ shows that costs were inflated (ucla.app.box.com)
- ^ noncash depreciation cuts into their profits (journals.sagepub.com)
- ^ A 2004 report (www.govinfo.gov)
- ^ profit margins for the nursing home industry would jump (doi.org)
- ^ Government Accountability Office has found (www.gao.gov)
- ^ Click to learn more about how some existing tools (theconversation.com)
Authors: Sean Campbell, Investigative journalist, The Conversation